A Complicated Case in 3 Parts
The Complicated Cases…Can sometimes turn out to be just following the dots to a next level using all that you already know.
I have been working intensively on a young man with serious pain problems in his right hip and left shoulder. Some of what’s needed was straight out of Mod 2 but taking a long time to change. Why? Because he has a couple of old injuries, one at T12/L1, from playing baseball as a kid that undermine the stability of corrections.
Part 1
Yesterday he came in with kyphosis of L1, 2 where there should be lordosis. What will lead me to understand what I haven’t addressed yet? Q: What supports the thoraco lumbar junction in the transition to lordosis? A: 2 things: Psoas and the Lumbar Erector group. I tested the lower branches of the Left Psoas that attach at L3 against the upper that attach at T12. The left L3 Psoas fibers inhibited the T12 fibers on both sides! I corrected these and released the excessively tight fibers of the Multifidi at T12/L1 on the left as the other key piece here was Left back extension inhibiting right side bending and right back shoulder.
The solution to the problem turned out to be an easy extrapolation of Mod 1 material, breaking down the Psoas into discreet segments.
In NMR Mod 1, we build stability with the big muscles first and then dial down for details to recreate a functional support system for the low back and hips. Even with Mod 1 NMR you will be able to address very complex low back and hip problems, one piece at a time….!

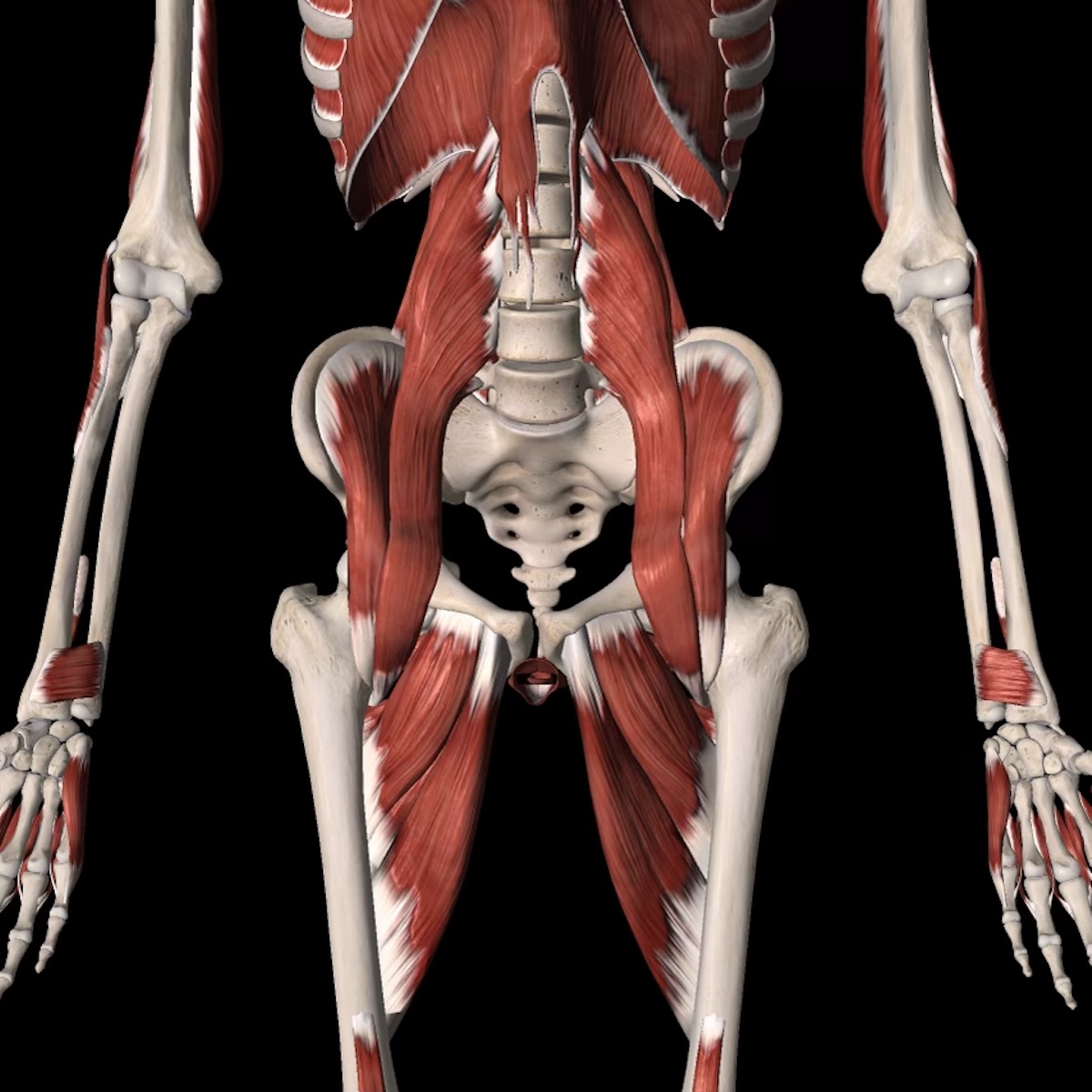
Psoas
Part 2
Today when he came in I had a chance to recheck the work I’d done on the 28th. The rotational coherence of his lumbar spine was holding. But once again both his Psoas muscles were weak. This is usually a sign of a rotated vertebra(e) between T12 and L3. Not today. That problem has stabilized. Something was definitely pulling his left leg on too tight. Here’s what I found:
His pain comes back first in the area of the right groin, then it involves his left shoulder. Tempting to work on the right groin. But left Iliacus was inhibiting left external hip rotation, left back extension, both Psoas muscles, and the right Lower Trapezius! After sorting out the hips I checked in at the left shoulder. it was rolled forward, too much basal tone in Pec Minor which was constantly engaging to help the weak right groin. Because it is leading contralateral movement for walking, it ends up inhibiting the muscles it is compensating for.
Left hip strong and tight; right hip weak and strained. I did no work on the right hip although that is where the pain is. Only the left hip and the left shoulder. All pain gone for now… to be continued…
BTW, this young man had been 10 years on opiates to handle his pain. NMR got him well enough organized that he was able to make a move to stop using them. He has now successfully withdrawn from all pain meds. That was another horror story. Please keep your kids OFF pain meds. Oxycodone is the worst. It has now been approved for kids as young as 11 years old. Criminal! So addictive; horrendous path to get off these things.
Anatomical illustration of Psoas Minor I wonder if it was contributing to the right side lean of the spine? Stay tuned and we’ll find out.
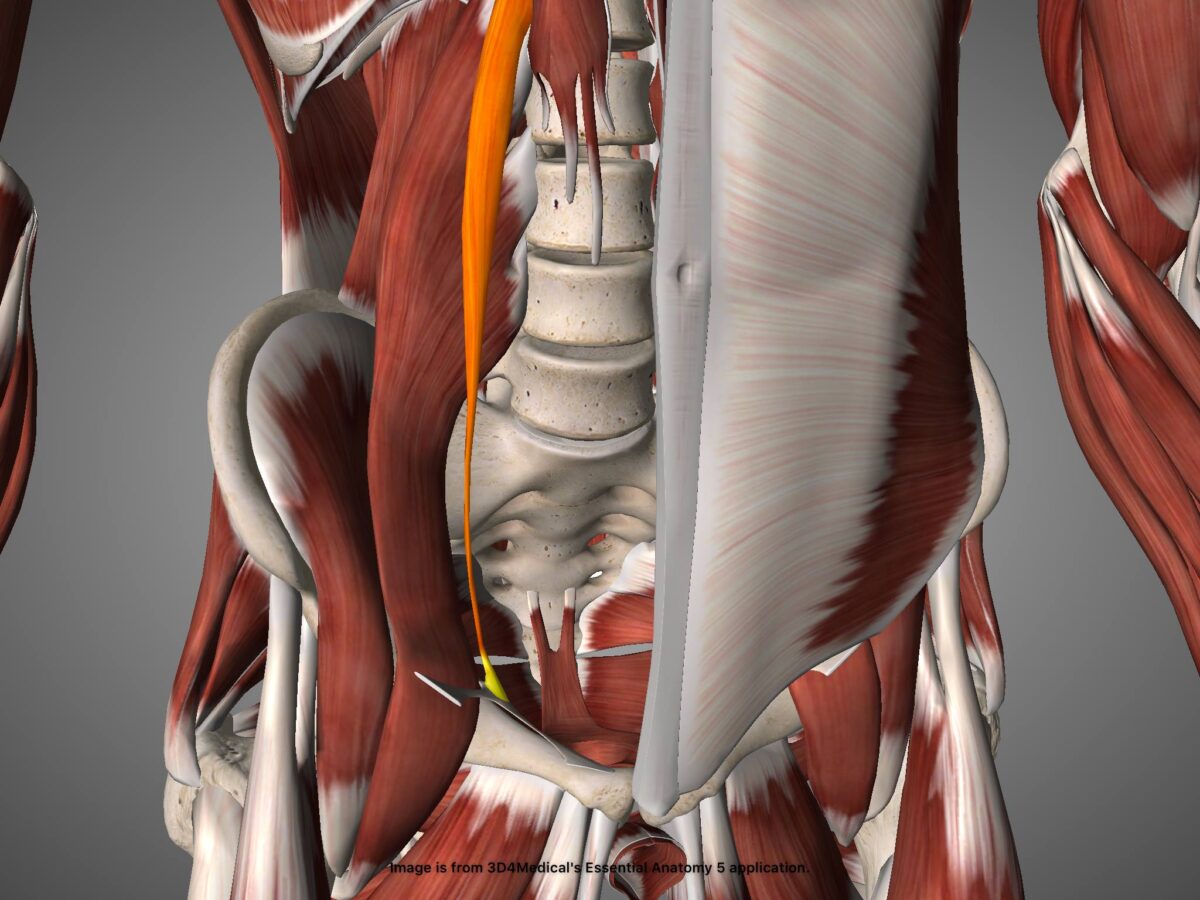
Psoas Minor
Part 3
I like to set up experiments for myself in sessions, especially on clients whose problems are largely resolved but some core pattern keeps coming back and back. In this way I am always learning new things, from the bodies I work on.
NMR gives us a way of testing theories and connections and discovering and developing new understandings.
I work with the premise that if there is still tissue abnormality there is coordination dysfunction. This may seem over simplified but gives a good rule of thumb that you’re not done if everything is not acting normal. To be continued next week…
My young client who’s issues with Psoas muscles that wouldn’t stay strong came back in today. His right groin was experiencing its characteristic ache; all fibers of the Iliacus inhibited. His left shoulder was inhibited for rotation in both directions.
His L4/5 was rotated left**
We de-rotated L4/5 to the right. His right groin got strong and his left shoulder recovered its integrity. Instability at L4/5 is key for him, it’s the king pin of all his problems. Instead of being a groin problem and a shoulder problem (although there was plenty to sort out there), it is really all just fallout from the instability in rotation at the bottom of the pillar of the spine.
I sent him across the hall to talk to an Orthopod about Prolotherapy injections for the unstable ligaments at L4/5.
**Observation: (Psoas will be ‘on’ on the opposite side to lumbar rotation preference, and off on the left side in this case.)